Two systematic reviews on FES cycling for stroke were published in early 2026, both by Alashram and colleagues, and both have made the conversation about FES cycling in stroke considerably more interesting. One reviewed the evidence for gait outcomes. The other reviewed the evidence for balance. Together, they cover most of what a stroke physio is asked about when a patient or family enquire about FES cycling. The headlines from both reviews push back against some of what the rehabilitation industry has long implied.
If you are a stroke physio working in an NHS community team, an early supported discharge service, or a neuro outpatient clinic, the question is not whether FES cycling has a place in stroke rehabilitation. It does. The question is where, for whom, and against what realistic outcome expectations.
The answer in May 2026 is that FES cycling has a defensible niche in stroke care. It is a smaller, more specific niche than vendor materials sometimes imply, and it is a different niche from the one many of us assumed five years ago. The recent reviews force the conversation to be more precise.
What the 2026 Evidence Says
Two reviews to anchor against.
The gait review, Alashram 2026 in Physiotherapy Research International, pooled ten randomised controlled trials with 311 participants. Across the 10-metre walk test, the 50-metre walk test, and the 6-minute walk test, the pooled effects were small and statistically non-significant. The authors describe the evidence as "limited" and "inconclusive" and do not recommend FES cycling to improve gait outcomes after stroke based on the current evidence. The methodological quality of the included trials was reasonable; the limitation lies in the size and consistency of the evidence base, not in the trials themselves.
The balance-related review, Alashram 2026 in Artificial Organs, pooled nine RCTs with 285 participants. The Trunk Control Test showed a non-significant favourable trend. The Berg Balance Scale showed a statistically significant pooled effect favouring control comparators over FES cycling, SMD -0.52 (95 per cent confidence interval -0.97 to -0.08). That is not the same as "FES cycling does nothing for balance"; it means that, in trials where the comparator was a balance-specific intervention, the balance-specific intervention did better. That is a useful finding. It tells us that if balance is the primary goal, balance-specific training is the better-evidenced choice.
These are not encouraging headlines for vendors. They are useful headlines for clinicians. We now have a clearer picture of where FES cycling does and does not earn its place in a stroke pathway.
Where the Evidence Does Support FES Cycling After Stroke
A third 2024 review, by Galvão and colleagues in BioMedical Engineering OnLine, asked a different question and got a more positive answer. They restricted their inclusion to early subacute stroke and to trials in which FES cycling was added to an exercise programme rather than tested in isolation. Across five RCTs in 187 patients, two findings stand out.
Trunk control improved by an average of nine points on the Trunk Impairment Scale, exceeding the minimum detectable change of around 3.5 points. Walking distance on the 6-minute walk test improved by an average of 95 metres, exceeding the minimal detectable change of about 61 metres in subacute stroke. Both findings carried moderate-quality GRADE evidence.
It is worth pausing on what this means. In early subacute stroke, when FES cycling is delivered as part of a structured exercise programme rather than as a standalone intervention, there is moderate-quality evidence for clinically meaningful improvements in trunk control and walking endurance. Walking speed, ADL scores, and the Motricity Index were similar to exercise alone in the same review. So the picture is specific: subacute, additive, trunk and endurance, not speed or ADL.
The other piece of recent evidence worth attention is Descollonges and colleagues, published in the Journal of NeuroEngineering and Rehabilitation at the end of 2025. This was not a meta-analysis but a controlled within-subject crossover in 15 post-stroke patients at a mean of 148 days post-stroke. Participants completed a session of FES-assisted cycling and a session of traditional cycling at the same workload. The cardiovascular response was similar across conditions; heart rate, end-tidal CO2, cardiac output, and middle cerebral artery blood flow velocity all increased comparably in both conditions. Perceived effort, however, was substantially lower during FES-assisted cycling. The effect size for perceived effort was very large.
I should note that several authors of that paper are affiliated with Kurage, the FES system manufacturer used in the trial. The finding is plausible and methodologically clean, but the conflict of interest is worth disclosing.
The implication of Descollonges is the practical one we should take seriously. It is not that FES cycling produces a different cardiovascular dose; rather, it appears to deliver the same cardiovascular dose at lower perceived effort, which is a real adherence advantage for a population in which perceived effort is one of the main barriers to exercise participation. For a stroke physio who has spent a session trying to talk a deconditioned patient through one more minute on an arm crank or recumbent bike, this is a meaningful finding.
The hybrid FES cycling literature, summarised in Máté and colleagues' 2023 review in Archives of Physical Medicine and Rehabilitation, also presents a distinct cardiovascular argument.
Hybrid FES cycling, where leg FES is combined with arm cranking, produces moderately greater oxygen uptake than arm cranking alone and substantially greater oxygen uptake than FES cycling alone. Longitudinal hybrid training improves aerobic fitness with a moderate-to-large effect. Most of that literature is from the SCI population, but the included stroke evidence points the same way.
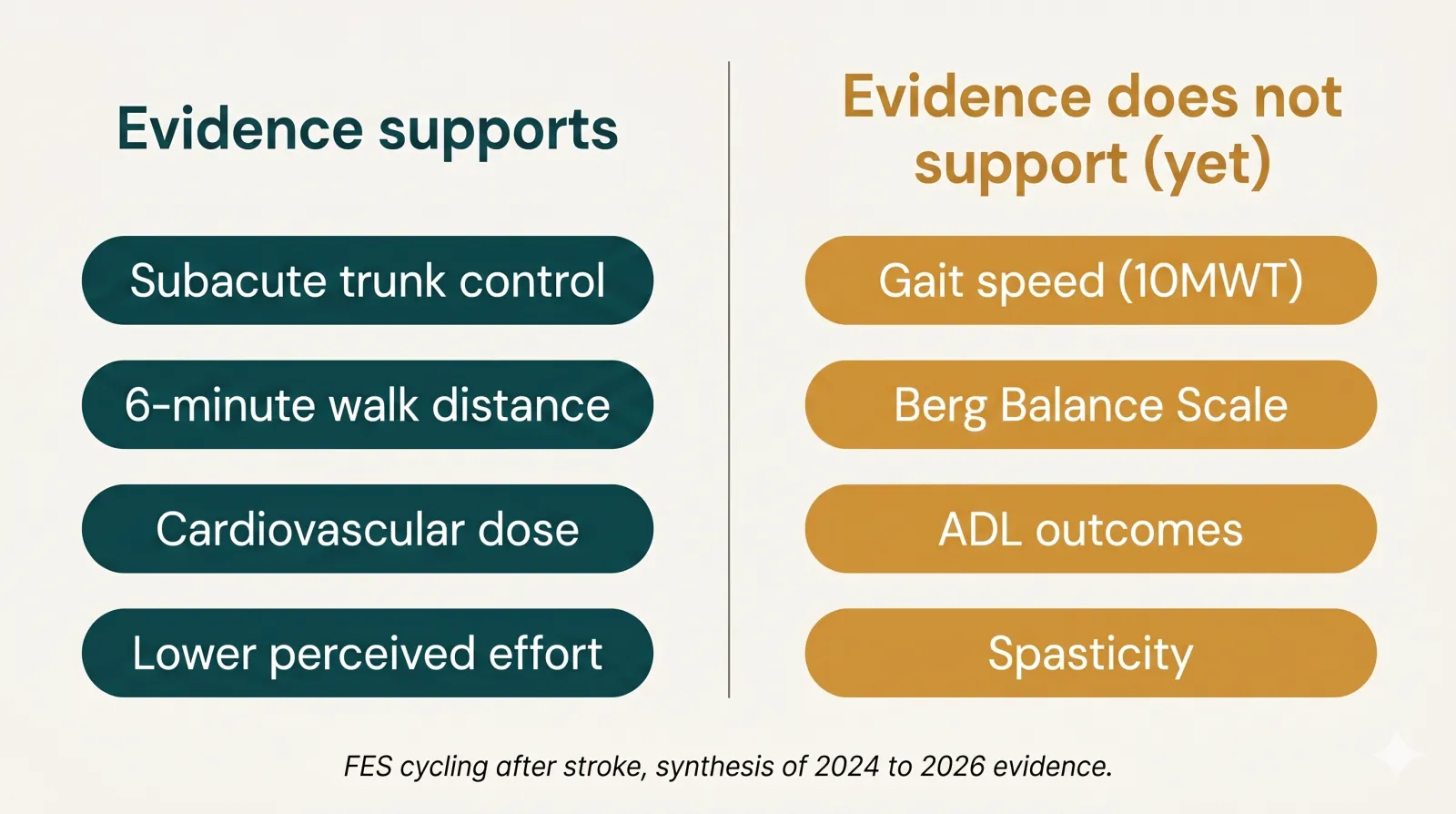
So the defensible position is this. FES cycling, in stroke, has moderate-quality evidence for early subacute trunk control and walking endurance when combined with an exercise programme. It has good evidence for delivering a cardiovascular dose at a lower perceived effort. It has emerging evidence for hybrid arm-leg cycling as a cardiovascular conditioning tool. It does not have evidence for improving gait speed, Berg balance scores, ADL outcomes, or spasticity in stroke specifically.
That is a narrower, more useful position than the broader claims sometimes made.
The Dose Problem
One observation from the reviews is worth flagging because it affects how stroke physios design programmes. Most stroke FES cycling trials run for three to eight weeks. Galvão's review notes that the recommended minimum dose for mobility outcomes in stroke rehabilitation is around twelve weeks. By that standard, the published stroke FES cycling literature is, for the most part, underdosed.
This matters for two reasons. First, when a review concludes that the evidence is "limited" or "non-significant," some of what it is observing is the limitation of the dose, not necessarily the limitation of the intervention. Second, when designing a clinical programme rather than a trial, twelve weeks of three to four sessions per week is a more suitable starting point than the three- to eight-week protocols that dominate the literature.
Stimulation parameters across the trials with positive findings cluster reasonably tightly. Frequencies typically 30 to 40 Hz, pulse widths 300 to 400 microseconds, three or more muscle groups stimulated (commonly hip extensors, knee flexors and extensors, dorsiflexors, plantar flexors), resistance progressively loaded to around 50 per cent of peak power output where measured. Sessions of 20 to 30 minutes, three to six per week. Patients with moderate to severe paresis tolerate this intensity, but those with very mild impairment show smaller effects, largely because the outcome scales reach ceilings quickly.
The biggest single-dose lesson is that FES cycling alone is not the ideal intervention. FES cycling on top of an exercise programme, in a patient who can sit upright for thirty minutes, in early subacute phase, with sessions delivered consistently across at least twelve weeks, is the appropriate intervention. The literature is reasonably clear about this.
Who Tends to Respond
The trials with the cleanest positive findings include patients in early subacute phase, typically between seven days and three months post-stroke, with moderate to severe lower-limb paresis but enough cognitive engagement and sitting tolerance to participate in twenty to thirty minutes of training. Patients initially unable to walk, perhaps surprisingly, may be among the better responders. The Ambrosini 2019 RCT in the European Journal of Physical and Rehabilitation Medicine found that 91 per cent of moderate-to-severe gait-impaired patients in the FES biofeedback arm achieved a clinically meaningful change in gait speed, against 36 per cent of controls (p = 0.008), even though the overall trial did not reach statistical significance.
Common exclusions across trials carry across to clinical decisions. Significant cognitive impairment that limits engagement, joint contractures that prevent pedalling, uncontrolled cardiovascular disease, a pacemaker or implanted electronic device without specialist clearance, pregnancy, active deep vein thrombosis, lower-limb skin breakdown over electrode sites, or uncontrolled epilepsy. These should sit on every screening checklist.
Chronic stroke is a different proposition from many of our clients who are recovering from a spinal cord injury. The evidence base in chronic stroke FES cycling is sparser and more mixed. That does not mean chronic stroke patients should not be considered, particularly where deconditioning is the limiting factor for further rehabilitation participation, but the evidence-based case is harder to make than in early subacute stroke.
Where FES Cycling Sits Alongside the Alternatives
Treadmill training and body-weight-supported treadmill training have moderate-quality Cochrane-level evidence, particularly when delivered with electromechanical assistance, for improving walking ability in non-ambulatory subacute stroke. Robot-assisted gait training has similar evidence. Both target task-specific gait, which FES cycling does not.
FES walking systems, dropfoot stimulators (ODFS, WalkAide, and equivalents), and multi-channel walking systems are different interventions from FES cycling. The evidence base is strongest for stroke FES and supports both an orthotic effect (immediate gait improvement when worn) and a quite modest therapeutic effect (some carryover when not worn). If your patient's primary functional limitation is foot drop during gait, a dropfoot stimulator is the more direct intervention.
Conventional cycle ergometry without stimulation is perhaps the natural comparator. The Descollonges 2025 finding suggests FES cycling adds value not by producing a different cardiovascular response but by making the same response feel less effortful, which translates into adherence and tolerated dose.
rTMS and tDCS adjuncts are upstream interventions targeting cortical excitability. They are complementary to FES cycling rather than competitive with it. Combined protocols are an active area of research, but no high-quality stroke trials of FES cycling combined with non-invasive brain stimulation have yet been reported.
The summary is that FES cycling is a complement, not a replacement, for the established stroke rehabilitation toolkit. Where it earns its place, it earns it on cardiovascular conditioning, adherence, trunk control and walking endurance, in combination with conventional rehabilitation rather than instead of it.

When to Choose FES Cycling, and When to Choose Something Else
For a stroke physio reading the 2026 evidence, four practical positions stand out.
FES cycling is a good choice for an early subacute stroke patient with moderate-to-severe lower-limb paresis, when the clinical goals are to deliver an active aerobic dose, recover trunk control, and build walking endurance, alongside conventional rehabilitation. The Galvão evidence supports this directly.
It is also a good choice for a deconditioned stroke patient at any phase, when sustained voluntary cycling with a passive/active bike cannot deliver an adequate aerobic dose. The Descollonges evidence supports the adherence argument, and the broader literature on hybrid FES cycling and cardiovascular conditioning supports the conditioning case.
It is not the strongest choice if the primary goal is to improve gait speed on the 10m walk test. The 2026 Alashram pooled evidence does not support that claim, and treadmill training, robot-assisted gait training, or task-specific gait practice are likely to be more effective.
It is not the strongest choice if the primary goal is Berg balance score improvement. The 2026 Alashram balance review found a pooled effect favouring control comparators, and balance-specific training is likely to do better.
For foot-drop correction during gait, FES cycling is not the relevant intervention; a dropfoot stimulator is.
For spasticity reduction, the evidence base for stroke FES cycling is insufficient; first-line management remains stretching, baclofen, and focal botulinum toxin, where appropriate. Although this reflects the evidence, in practice, we often find the effects of FES cycling worthy of consideration.
What you tell the patient and family about realistic outcomes should match the evidence. "You will likely tolerate a useful aerobic dose more easily than with traditional cycling." "You will recover trunk control faster than with exercise alone, in early subacute stroke." "You will walk further on the 6-minute walk test." All defensible. "You will walk faster." "Your Berg balance score will improve more than with conventional balance training." "Your spasticity will reduce." Not considered likely on the present evidence in stroke.
What's Coming
Two pieces of work to keep an eye on. The Cleveland Clinic ISCORE trial, with its protocol published in Physical Therapy in late 2025, is recruiting 66 subacute stroke patients to a twelve-week pragmatic RCT of facilitated cycling exercise plus abbreviated PT/OT against standard PT/OT, with EEG, blood biomarkers and a formal cost-effectiveness analysis. This is the first major stroke trial planning a proper economic evaluation of FES cycling.
The combination of FES cycling with non-invasive brain stimulation (rTMS or tDCS) is the most active area of research. There are no published high-quality stroke RCTs of these combined protocols yet, but the hypothesis (cortical priming combined with peripheral patterned activation) is biologically coherent and the early signals from related populations are interesting.
For Anatomical Concepts and the kind of work we do with stroke clients, the practical takeaway from these reviews is that the case for FES cycling rests on its narrower niche rather than on broad claims about gait recovery. It is on us to be precise about that with referrers and families.
Where to Go From Here
If you are a stroke physio considering FES cycling for a specific patient, the questions worth asking are these. Is the patient in the early subacute phase, or is deconditioning the dominant limitation? Is the goal cardiovascular dose, trunk control, or walking endurance, rather than gait speed or Berg score? Can the patient sit upright and engage for twenty to thirty minutes? Is there capacity to deliver a programme of at least twelve weeks at three to four sessions per week, alongside conventional rehabilitation? If the answer to those is mostly yes, FES cycling could have a place in the plan.
If you would like to talk through a specific patient or service question, please get in touch.
The 2026 evidence has narrowed the claims FES cycling can defensibly make in stroke. The claims it can still make are real, and they matter.
Further Reading
- Alashram AR. Functional Electrical Stimulation Cycling for Gait Rehabilitation in Stroke Survivors: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Physiotherapy Research International 2026;31(2):e70188. https://doi.org/10.1002/pri.70188
- Alashram AR. Functional Electrical Stimulation Cycling for Balance Rehabilitation in Stroke Survivors: A Systematic Review and Meta-Analysis. Artificial Organs 2026. https://doi.org/10.1111/aor.70116
- Galvão WR et al. Cycling using functional electrical stimulation therapy to improve motor function and activity in post-stroke individuals in early subacute phase: a systematic review with meta-analysis. BioMedical Engineering OnLine 2024;23(1):1. https://doi.org/10.1186/s12938-023-01195-8
- Descollonges M et al. Positive effects of functional electrical stimulation-assisted cycling on perception of effort, cerebral blood flow and cognition in post-stroke patients. Journal of NeuroEngineering and Rehabilitation 2025;22(1):257. https://doi.org/10.1186/s12984-025-01800-y (Note: several authors affiliated with Kurage, the device manufacturer.)
- Máté S et al. Hybrid FES cycling and oxygen uptake in central nervous system disorders: systematic review and meta-analysis. Archives of Physical Medicine and Rehabilitation 2023;104(11):1928-1940. https://doi.org/10.1016/j.apmr.2023.03.026
- Ambrosini E et al. Multimodal biofeedback FES-cycling and balance training in subacute stroke: an RCT. European Journal of Physical and Rehabilitation Medicine 2020;56(1):24-33. https://doi.org/10.23736/S1973-9087.19.05847-7
- Miller CR et al. ISCORE trial protocol: Improving Stroke COgnitive REcovery through facilitated cycling exercise. Physical Therapy 2025;105(12). https://doi.org/10.1093/ptj/pzaf139