If you have been living with MS for any length of time, you will probably have learned, often the hard way, that some kinds of exercise leave you wiped out for the rest of the week. So when someone suggests adding electrical stimulation to a cycling session, the obvious reaction is: that is the last thing I need.
I understand that reaction. In my experience, it is a reason people with MS turn down the chance to try FES cycling, even when their neurologist or therapist has raised it. The lived knowledge that exercise can make symptoms worse for days afterwards is real, well evidenced, and should not be brushed aside.
The argument I want to make is narrower than the claim that "exercise is good for MS." That argument has been settled for nearly thirty years. The argument here is that FES cycling appears to be mechanically different from voluntary exercise in ways that matter for people with MS, especially those whose mobility has progressed to the point where ordinary exercise has become unmanageable. The evidence for that claim is real but modest. I will tell you where it is solid and where it runs out.
Why exercise can make MS worse: the part nobody made up
The phenomenon has a name. It is called Uhthoff's phenomenon, first described in 1890 in patients whose vision blurred after exertion. The mechanism is now reasonably well understood. Partially demyelinated axons, as occur in MS, are temperature-sensitive: when core body temperature rises by even a small amount (Filingeri and colleagues showed measurable changes with a rise of around 0.4 degrees Celsius), nerve conduction in those axons slows or fails. The result is a transient worsening of vision, weakness, fatigue, and sometimes cognitive symptoms. Estimates put the proportion of people with MS who experience some form of Uhthoff's phenomenon at between 60 and 80 per cent.
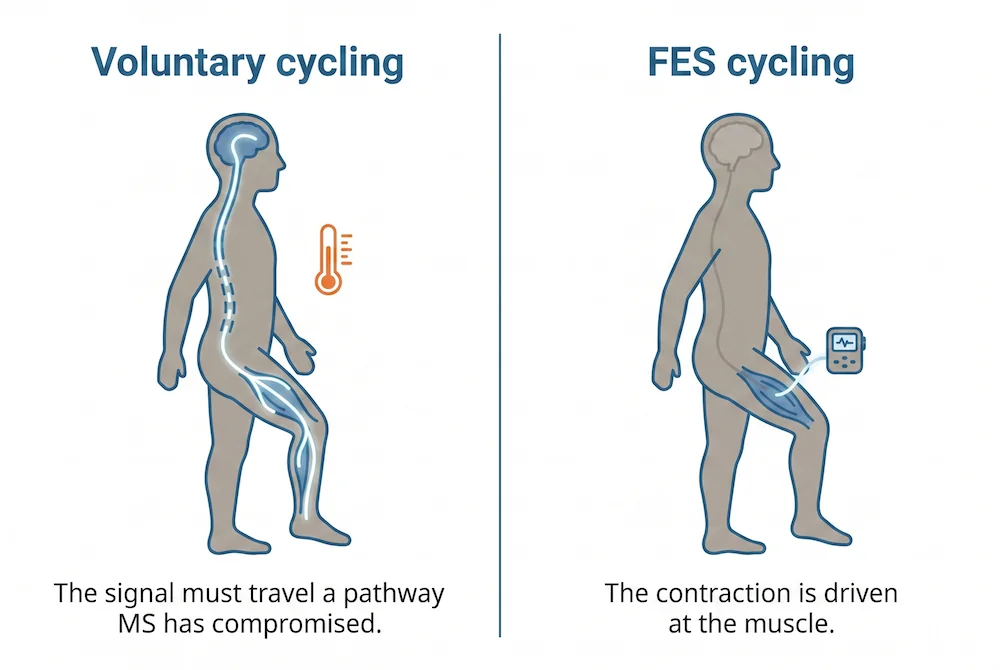
There is a second, related issue. MS-related fatigue is mostly central rather than peripheral. Coates and colleagues showed in 2020 that the most fatigued people with MS have measurably weaker corticospinal responses during exercise. In plain English, the bottleneck is not the muscle running out of 'fuel'. The bottleneck is the signal getting from the brain to the muscle in the first place. Voluntary exercise asks more of exactly the system that MS has compromised.
Put those two together (heat sensitivity in damaged axons, plus a corticospinal tract already at the edge of its capacity) and the lived experience of "exercise makes me worse" stops being a complaint and starts being a description of the actual physiology.
The advice changed thirty years ago
For decades, people with MS were told to rest. That advice was overturned in 1996 by a randomised trial led by Petajan and colleagues, which showed that aerobic training improved fitness and quality of life without worsening neurological status. The literature has since piled in behind that finding. The most recent meta-analysis I could find (Learmonth and colleagues, 2023) pooled 40 randomised trials with 1,780 participants and concluded that exercise training does not increase the risk of relapse, of any adverse event, or of any serious adverse event.
The summary of where the field has landed is that exercise is not the enemy. Heat and central drive are. Anything that delivers a training stimulus while keeping a lid on those two things is, in principle, the form of exercise that should suit MS best.
This is where FES cycling enters the conversation.
What FES cycling actually does, and why it is different
In FES cycling, electrical stimulation makes the peripheral muscles contract. The cortex does not have to issue the command for the individual to deliver each pedal stroke; that's what the stimulator does. This is the entire premise of FES, and it is the reason the modality has been used in spinal cord injury rehabilitation for decades. Applied to MS, it means a person can exercise the leg muscles without relying on the corticospinal pathway, which fatigue has already pushed to the limit.
The clearest published evidence for "different demand on the system" comes from Edwards and colleagues at the University of Ottawa, working with the Pilutti group. In a 2026 study comparing FES leg cycling, arm crank, and recumbent stepper at matched perceived effort in advanced MS, FES cycling produced significantly lower oxygen consumption, heart rate, and work rate while still remaining within the moderate-to-vigorous training zone. The authors expressed the situation as follows:-
"At a matched RPE, FES cycling may provide a less demanding aerobic stimulus."
FES cycling is not effortless. But for the same subjective level of exertion, it costs the body less. That is the distinction the literature can now support.
A related finding comes from Reynolds and colleagues in 2014. Using near-infrared spectroscopy to measure muscle oxygen consumption in non-ambulatory people with MS before and after a four-week FES cycling programme, they recorded an average increase of 47 per cent. The muscles were getting healthier, even in people whose voluntary movement had largely gone.
The trial evidence on fatigue, walking, and quality of life
There are only a small number of randomised trials of FES cycling in MS, and the sample sizes are small. Let me walk through the most defensible ones rather than claim more than the evidence supports.
The Pilutti and Edwards group ran a pilot RCT published in 2018. Some 11 people with moderate-to-severe MS (EDSS 5.5 to 6.5) were randomised to FES cycling or passive leg cycling three times a week for 24 weeks. Adherence was good, no serious adverse events, and the FES group showed a 22.9 per cent improvement in the timed 25-foot walk and a 13.8 per cent improvement in peak oxygen consumption compared to passive cycling.
A follow-up paper from the same trial, published in 2019, looked at fatigue, pain, and cognition. The Fatigue Severity Scale showed a large effect favouring FES cycling. The Modified Fatigue Impact Scale showed a moderate effect. Pain dropped. The Symbol Digit Modalities Test, which measures cognitive processing speed, showed a clinically meaningful improvement. The sample is too small to call this proven, but the direction of every measure was the same.
The Backus group at the Shepherd Center published their own trial in 2020 with twenty-one randomised participants (EDSS 7.0 to 8.5, all wheelchair-using). Twelve completed the twelve-week programme and showed moderate-to-large favourable effects on fatigue, depression, and physical-health quality of life.
A UK-led systematic review by Scally and colleagues in 2019 (University of the West of Scotland) pulled together nine studies. Their summary was characteristically British: "FES cycle training appears to be well tolerated in PwMS with mobility impairment, with no serious adverse events," followed by the appropriate caution that "the low quality of the literature precludes any definitive conclusions."
That is the evidence picture. It is not a stack of large multi-centre trials. It is a consistent set of small studies, none of them industry-funded, all pointing in the same direction.
The UK context, briefly
It is worth knowing where this sits in UK clinical guidance. NICE has accepted FES for MS-related drop foot since 2009 (IPG278), and the 2022 MS management guideline (NG220) actively encourages exercise. Neither document directly addresses FES cycling for MS, which means in practice it is not on the standard NHS pathway and is generally accessed privately or through case-managed care.
The MS Society's own 2022 evidence pack on FES (which again deals primarily with drop foot rather than cycling) makes a separate point worth flagging. Even for the indication NICE has approved, around four out of every five people with MS who would like FES are not getting it. Access is patchy, postcode-dependent, and frustrating. That is the context in which most of our clients arrive at the conversation.
Starting carefully: a protocol that respects the fatigue concern
If you decide to try FES cycling and are heat-sensitive or new to electrical stimulation, published trials suggest a starting pattern that is much gentler than most product brochures imply.
In the studies that built up tolerance carefully (Williams and colleagues 2020 in particular), participants started at as little as three to five minutes of total cycling, in a cool environment, with a fan running, and built up over two to four weeks toward thirty minutes. Symptoms (vision changes, unusual weakness, tingling) were monitored not just during the session but for twenty-four hours afterwards. No serious adverse events were reported across the protocols tested.
In our experience, that conservative pattern is not just a safety measure. It is the way to find out, honestly and on your own terms, whether your nervous system tolerates the modality. If FES cycling is going to suit you, you will know inside the first three or four sessions, and you will not have spent a week wiped out finding out.
What FES cycling will not do
Here are the claims the evidence does not yet support.
It does not slow MS disease progression. It does not reduce the relapse rate. There is no published trial showing it changes the EDSS (Expanded Disability Status Scale) over time. The cognitive signal from the Pilutti 2019 paper is encouraging but rests on a handful of completers, and replication is not yet there.
It is also not the only form of exercise people with MS can tolerate. Cool-water swimming, recumbent stepping, and arm ergometry are sensible alternatives, especially earlier in the disease course. FES cycling earns its keep in the EDSS 5.5 and above territory, where voluntary leg exercise has become difficult or unsafe.
A practical next step
If you are sceptical, the next right step is to try the modality in a controlled setting, with someone who can adjust the parameters around your fatigue threshold rather than a textbook protocol.
That is what an assessment is for. In our case, it means a session in a cool room, a sensible, modest starting dose, electrodes adjusted around your spasticity pattern, and a conversation about whether your particular MS picture is one where FES cycling is likely to help. Sometimes the answer is yes. Sometimes it is "not yet, the priority is something else." Either is a useful answer.
The fear of pushing too hard and crashing for three days is not paranoia. It is the appropriate caution of someone who has learned what their body does. FES cycling does not override that caution. Done properly, it works with it.
If you would like to find your own threshold without committing to a system, please get in touch. We will walk through your situation and tell you whether a demonstration session is the right next step, or whether something else should come first.
Further Reading
Backus D, Moldavskiy M, Sweatman WM. Effects of functional electrical stimulation cycling on fatigue and quality of life in people with multiple sclerosis who are nonambulatory: a randomized controlled trial. International Journal of MS Care. 2020. https://doi.org/10.7224/1537-2073.2019-101
Coates KD, Aboodarda SJ, Krüger RL, Martin T, Metra A, Newans T, et al. Multiple sclerosis-related fatigue: the role of impaired corticospinal responses and heightened exercise fatigability. Journal of Neurophysiology. 2020. https://doi.org/10.1152/jn.00165.2020
Edwards T, Motl RW, Sebastião E, Pilutti LA. Pilot randomized controlled trial of functional electrical stimulation cycling exercise in people with multiple sclerosis with mobility disability. Multiple Sclerosis and Related Disorders. 2018. https://doi.org/10.1016/j.msard.2018.08.020
Edwards T, et al. Cardiorespiratory and perceptual responses to FES leg cycling, arm crank ergometry, and recumbent stepping at matched RPE in advanced multiple sclerosis. Multiple Sclerosis and Related Disorders. 2026. https://doi.org/10.1016/j.msard.2026.107065
Filingeri D, Chaseling G, Hoang P, Barnett M, Davis SL, Jay O. Afferent thermosensory function in relapsing-remitting multiple sclerosis following exercise-induced increases in body temperature. Experimental Physiology. 2017. https://doi.org/10.1113/EP086320
Jain A, Rosso M, Santoro JD. Uhthoff's phenomenon in multiple sclerosis. Multiple Sclerosis Journal. 2019. https://doi.org/10.1177/1352458519881950
Latimer-Cheung AE, Pilutti LA, Hicks AL, Martin Ginis KA, Fenuta AM, MacKibbon KA, Motl RW. Effects of exercise training on fitness, mobility, fatigue, and health-related quality of life among adults with multiple sclerosis: a systematic review to inform guideline development. Archives of Physical Medicine and Rehabilitation. 2013. https://doi.org/10.1016/j.apmr.2013.04.020
Learmonth YC, Herring MP, Russell DI, Motl RW, Pilutti LA. Safety of exercise training in multiple sclerosis: an updated systematic review and meta-analysis. Multiple Sclerosis Journal. 2023. https://doi.org/10.1177/13524585231204459
MS Society UK. FES Evidence Pack (Hentschel J). May 2022. https://www.mssociety.org.uk/sites/default/files/2022-05/FES%20Evidence%20Pack%20V3.pdf
MS Trust. A-Z entry: Functional Electrical Stimulation. https://mstrust.org.uk/a-z/functional-electrical-stimulation-fes
NICE. Multiple sclerosis in adults: management. NG220. June 2022. https://www.nice.org.uk/guidance/ng220
NICE. Functional electrical stimulation for drop foot of central neurological origin. IPG278. 2009. https://www.nice.org.uk/guidance/ipg278
Petajan JH, Gappmaier E, White AT, Spencer MK, Mino L, Hicks RW. Impact of aerobic training on fitness and quality of life in multiple sclerosis. Annals of Neurology. 1996. https://doi.org/10.1002/ana.410390405
Pilutti LA, Edwards T, Motl RW, Sebastião E. Functional electrical stimulation cycling exercise in people with multiple sclerosis with mobility disability: secondary outcomes from a pilot randomized controlled trial. International Journal of MS Care. 2019. https://doi.org/10.7224/1537-2073.2018-048
Reynolds MA, McCully KK, Burdett B, Manella C, Hawkins L, Backus D. Pilot study: evaluation of the effect of functional electrical stimulation cycling on muscle metabolism in nonambulatory people with multiple sclerosis. Archives of Physical Medicine and Rehabilitation. 2014. https://doi.org/10.1016/j.apmr.2014.10.010
Scally JB, Baker JS, Rankin J, Renfrew L, Sculthorpe N. Evaluating functional electrical stimulation (FES) cycling on cardiovascular, musculoskeletal and functional outcomes in adults with multiple sclerosis and mobility impairment: a systematic review. Multiple Sclerosis and Related Disorders. 2019. https://doi.org/10.1016/j.msard.2019.101485
Williams J, Burdett B, Hawkins L, Manella C, Backus D. Safety and tolerance of varied exercise protocols using functional electrical stimulation cycling in non-ambulatory persons with multiple sclerosis. Archives of Rehabilitation Research and Clinical Translation. 2020. https://doi.org/10.1016/j.arrct.2020.100045